



Suboxone helps people with opioid use disorder by doing two things at once: calming the cravings and withdrawal that drive continued use, while making it hard to misuse the medication itself. It manages that through two ingredients, buprenorphine and naloxone, that each play a specific role.
Understanding how it works takes a lot of the fear out of starting it, so here is the plain-language version, from the chemistry to what treatment actually looks like week by week.
What Is in Suboxone
Suboxone combines buprenorphine and naloxone in a film or tablet that dissolves under the tongue. It comes in four strengths, from 2 mg of buprenorphine with 0.5 mg of naloxone up to 12 mg with 3 mg, and your prescriber selects and adjusts the strength based on how you respond. Buprenorphine is the active treatment. Naloxone is there mainly to discourage misuse. When the medication is taken as directed, buprenorphine does nearly all of the work.
How Buprenorphine Works
Buprenorphine is a partial opioid agonist. It attaches to the same brain receptors as heroin, fentanyl, and prescription opioids, but it activates them only partway. That partial activation is enough to switch off cravings and withdrawal without producing the full high of other opioids.
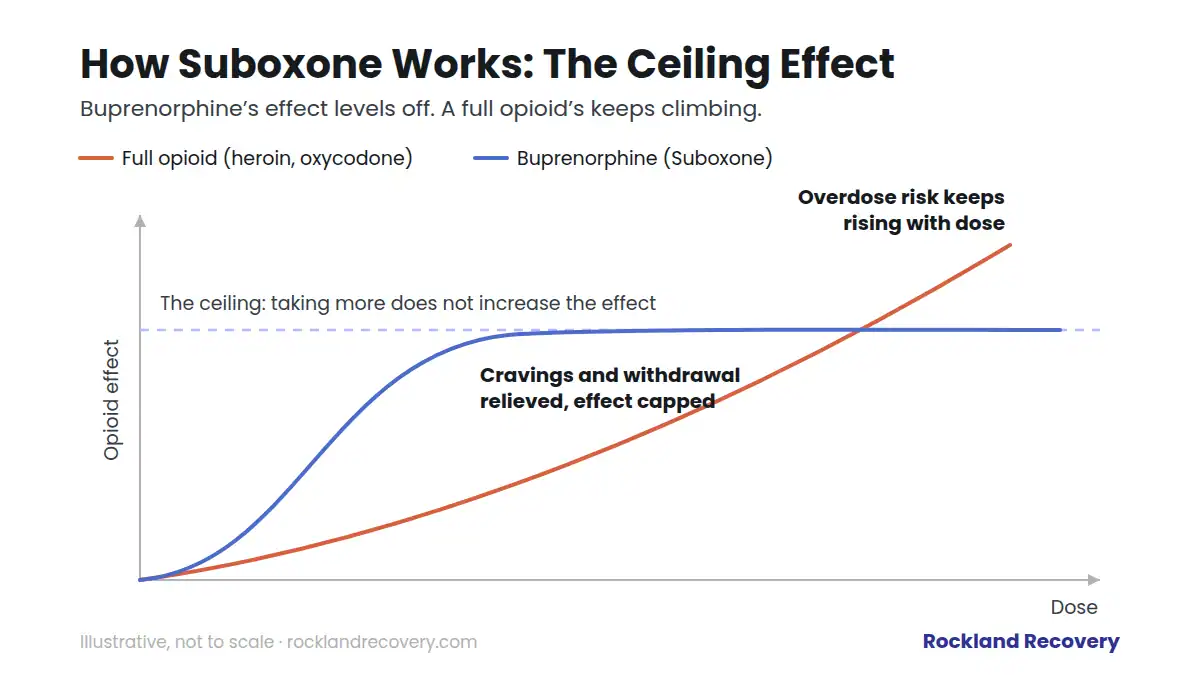
Two properties make it unusually well suited to this job. The first is its ceiling effect: past a certain dose, taking more buprenorphine does not increase its effect. That ceiling is a major safety feature, because it limits how much the medication can slow breathing, which is what makes full opioids deadly in overdose. The second is how tightly and how long it binds. Buprenorphine holds onto opioid receptors more strongly than most opioids and stays active in the body for a long time, which is why a single daily dose holds steady for a full day and why other opioids taken on top of it have little effect.
What the Naloxone Does
Naloxone is an opioid blocker, the same medication used to reverse overdoses. In Suboxone, it is included as a safeguard. Taken correctly under the tongue, very little naloxone is absorbed and it stays essentially inactive. If someone tries to misuse Suboxone by injecting it, the naloxone becomes active and can bring on withdrawal instead of a high. It is a built-in deterrent rather than part of the day-to-day treatment.
How Suboxone Eases Cravings and Withdrawal
When someone with opioid dependence stops using, the brain, having adapted to constant opioids, goes into overdrive and produces withdrawal. Buprenorphine settles onto those same receptors and quiets that reaction. Cravings ease, withdrawal symptoms fade, and the constant pull toward using loosens its grip. That relief is what frees a person to focus on counseling, work, relationships, and the rest of recovery.
People starting Suboxone often expect to feel medicated. Most describe the opposite: feeling normal for the first time in a long time. At a stable therapeutic dose there is no high and no sedation, just the absence of the noise that opioid dependence creates.
What the Research Shows
Buprenorphine is one of the best-studied medications in addiction treatment, and the findings are consistent. People taking it stay in treatment at higher rates than people in counseling alone, use illicit opioids less, and, most importantly, die less often. Studies following people in and out of treatment find the risk of fatal overdose drops by roughly half while someone is on buprenorphine. That is why SAMHSA and other leading health authorities consider it a first-line treatment for opioid use disorder rather than a fallback.
The same research carries a warning worth taking seriously: the risk concentrates around stopping. Leaving treatment early, or stopping abruptly, is when relapse and overdose risk spike. This is a medication that rewards patience.
The Three Phases of Suboxone Treatment
Phase 1: Induction (the first days)
Suboxone is not started at the peak of use. Because buprenorphine binds so tightly, taking it too soon after another opioid can push that opioid off the receptors all at once and trigger precipitated withdrawal, which comes on fast and hard. To avoid this, the first dose is timed for when you are already in early withdrawal, typically 12 to 24 hours after short-acting opioids, and it is guided by a provider. Done right, induction works quickly: most people feel withdrawal lift within an hour of a properly timed first dose, and the first days are spent finding the dose that holds you steady.
Phase 2: Stabilization (the first weeks)
Once withdrawal is controlled, the goal shifts to finding your maintenance dose, the amount that keeps cravings quiet for a full 24 hours without drowsiness. Your prescriber adjusts in small steps while you check in regularly. This is also when counseling begins in earnest, because the mental space the medication creates is exactly what therapy needs to work with.
Phase 3: Maintenance (months to years)
Maintenance is the long, quiet phase where recovery actually gets built inside a structured medication-assisted treatment program: steady medication, ongoing counseling, and a life that gradually stops orbiting around opioids. There is no fixed endpoint. Research favors staying on the medication while recovery stabilizes, often a year or more, and coming off it eventually happens through a slow, provider-guided taper rather than a stop date circled on a calendar.
Once you are stable, the medication stays in your system for days, not hours. If you are curious about that timeline, see our guide on how long Suboxone stays in your system.
Common Side Effects and How They Are Managed
Most side effects show up early and settle as your body adjusts. The frequent ones are headache, constipation, nausea, sweating, and trouble sleeping, and your prescriber has straightforward fixes for each, from timing adjustments to stool softeners. Some people notice numbness or tingling in the mouth where the film dissolves.
Two are worth flagging specifically. Dissolving buprenorphine medications can be hard on teeth over time, so the practical habit is to take a drink of water after the film fully dissolves, swish gently, and wait at least an hour before brushing. And the one genuinely dangerous combination is Suboxone with alcohol or benzodiazepines, which undercuts the ceiling effect’s protection against slowed breathing. That combination, not the medication alone, accounts for most serious problems, so be fully honest with your prescriber about everything else you take.
Who Suboxone Is For
Suboxone is for people with opioid use disorder, whether the opioid was heroin, fentanyl, or prescription painkillers like oxycodone and hydrocodone. It does not require hitting any particular bottom, and it works for people on their first attempt at recovery and people on their fifth. It is often the most practical choice for anyone coming directly off opioids, because it can be started in early withdrawal rather than after a week or more of abstinence.
It is not automatically the right choice for everyone. People with significant liver disease, people taking sedatives that interact with it, and people who simply want nothing opioid-based in their treatment may be better served by the alternative described below. Pregnancy does not rule out buprenorphine, but it does call for a prescriber experienced in treating opioid use disorder during pregnancy. This is exactly what the initial assessment is for.
Common Myths, Answered Briefly
“It’s just trading one addiction for another.” No. A steady therapeutic dose produces stability, not a high, and physical dependence on a prescribed medication is not addiction. We unpack this fully in our guide on whether Suboxone is addictive.
“You’re not really in recovery if you’re on medication.” The evidence says otherwise, and so do the years of rebuilt lives behind it. Recovery is measured in health, function, and connection, not in whether a medication helped you get there.
“It’s as dangerous as the opioids it replaces.” The ceiling effect and the naloxone were designed specifically to prevent that. Suboxone’s overdose risk is far lower than heroin, fentanyl, or prescription painkillers, with one caveat that matters: combining it with alcohol or benzodiazepines undermines those protections.
How Suboxone Compares With Other Options
Suboxone is one of two main medication approaches we offer for opioid use disorder. The other, Vivitrol, works in the opposite way: instead of partially activating opioid receptors, it blocks them completely. Each suits different situations, and the trade-offs are real enough that we wrote a full comparison in our Suboxone versus Vivitrol guide. For alcohol use disorder, a different set of medications applies, covered in our guide to medications for alcohol use disorder.
Suboxone Works Best as Part of a Plan
Medication handles the biology of opioid dependence, but recovery also involves the habits, triggers, and life circumstances behind it. That is why our medication-assisted treatment program in South Shore Massachusetts pairs Suboxone with counseling and support, alongside medically supervised detox when it is needed. To find out if it fits your situation, verify your insurance or call us at 855-732-4842.
Frequently Asked Questions
Is Suboxone an opioid?
Buprenorphine, its main ingredient, is a partial opioid. It activates opioid receptors only partway, with a built-in ceiling, which is what separates it from full opioids like heroin or oxycodone.
How long does Suboxone take to work?
Most people feel relief from withdrawal within an hour of the first properly timed dose. It is often used to calm early withdrawal quickly during induction.
How does Suboxone make you feel?
At a therapeutic dose, most people feel normal rather than high: cravings quiet down and withdrawal lifts, without the sedation or euphoria of other opioids.
Does Suboxone block other opioids?
Largely, yes. Buprenorphine binds tightly to opioid receptors, so it reduces the effect of other opioids taken on top of it. This is one reason not to combine them.
Can you overdose on Suboxone?
It is difficult at therapeutic doses because of the ceiling effect, but not impossible, especially if Suboxone is combined with alcohol or benzodiazepines. Taken alone and as prescribed, its overdose risk is far lower than full opioids.
How long do you stay on Suboxone?
There is no fixed answer. Some people benefit for months, others for years, and research favors staying on it while recovery stabilizes. The right length is a clinical decision made with your provider based on your progress.
This article is for general education and is not medical advice. Questions about Suboxone or starting treatment should go to a licensed provider who knows your history.